



“I don’t know.” Part 2.
Why diagnostic uncertainty deserves to be embraced by patients and doctors.

In Part 1, we covered what Diagnostic Uncertainty is, why it can be a good thing for you as a patient and for your doctor to express his doubts, and what you can do to encourage this level of openness and partnership. We also shared some real life stories of what can happen when there’s a lack of trust and respect between doctors and patients and how the physician’s discomfort with uncertainty can harm us.
In Part 2, let’s talk about why Diagnostic Uncertainty happens.
There are several reasons. Here are six:
Quantity and Complexity: In most cases, the diagnostic process follows an expected path. It may take an hour to a few weeks to get an accurate diagnosis based on physical exam, medical history and tests. But diagnosis can be a very intricate process.
Mark L. Graber, MD, FACP, a leader in identifying, defining, and fixing diagnostic errors, is the source of one of my favorite quotes about how complex medicine has become, perhaps too complex for an individual doctor to address without diagnostic tool support. “There are over 10 thousand diseases and only a few hundred symptoms,” he’s said many times. As of the latest version of MalaCards: The Human Disease Database, a project of the Weitzmann Institute of Science, there are almost 23 thousand disorders. There are new named diseases and medical conditions we didn’t know existed just a decade ago. It’s hard to diagnose a disease that has no name or known etiology.
A field of possibilities that large calls for a little humility and a lot of cooperation.Progression. Medical conditions change over time. They wax and wane, they worsen and improve, or they may start small and develop into something impossible to ignore. Sometimes, what you experience as a patient hasn’t progressed enough to be visible to the doctor, or evident in the blood tests, or the medical imaging (i.e., X-ray, CT scan, ultrasound). That’s another cause of diagnostic uncertainty. How can a physician pinpoint which of the 23 thousand disorders might be affecting you without clinical evidence?
That doesn’t mean you’ve been dismissed or ignored. Yet. At the end of that first appointment, when what you’re feeling isn’t observed by the physician, don’t forget to ask what to do if your symptoms get worse. You will most likely hear instructions to call and return if that happens.
I urge you to do so. And return with a careful and detailed description of your symptom’s progression. If you’re a subscriber, you can request a free copy of The Eight Characteristics of a Symptom. It’s an easy-to-follow checklist of how to describe your symptoms to a doctor the way they need to hear it. (Direct Message me.) That has been proven to help open a doctor’s mind and his differential.
If your worsened health is still dismissed, then it could be due to a different list of issues. Review this article about what to do if your doctor has dismissed you.A field of possibilities that large calls for a little humility and a lot of cooperation.
Heuristics: Medicine is a strange mix of science and educated opinion. Short of a broken bone or a deep cut on your finger, for example, diagnostic conclusions require educated opinion. That’s why your doctor has studied for eight to fifteen years. A correct diagnosis is their goal but it’s not guaranteed.
Some primary care doctors and specialists dislike admitting that. Professionals in all fields can be uncomfortable in the liminal state; that’s the place of ambiguity between one state and another, between the patient’s symptom reports and the correct answer and treatment. They feel pressured to come up with a fast answer. That answer will rely on their experience and statistics, at least at first.
Heuristics are mental shortcuts often used by physicians. They’re an approach to diagnosis that is pragmatic and rapid, based on assumptions and past experiences and are most often accurate. Let me stress that: most diagnoses are correct, even when heuristics are used. But not always.
Highly experienced experts in all fields use heuristics. Art experts may often identify a painting that’s been attributed to a master artist as a fake based on their gut first, then supported by a variety of tests. Doctors frequently do that with your health. If your child attends a school where 30 percent of the kids have come down with Fifth Disease and your kid has the typical red rash on their cheeks, your pediatrician will employ heuristics and diagnose him with Fifth Disease. However, there are at least ten other possible medical explanations for that red rash. Heuristics would stop the diagnostic process prematurely.Atypical presentations: What are considered typical presentations of many medical conditions are based on how otherwise healthy white men would present with that disease. That’s because most medical studies traditionally consisted of that one cohort. That’s changing for most new research studies which try to broaden the groups of people who participate. It’s still a problem for a long list of reasons which deserve their own column.
Meanwhile, everyone else –– women, Black, Asian and Hispanic patients, people with existing chronic illnesses and autoimmune conditions –– frequently present differently than otherwise healthy white men do. They still have that disease or condition; it’s just not showing up in the “expected” way. That’s when Heuristics just won’t do the job.
For example, most patients complaining of neck pain learn it’s most likely due to poor posture, lifting too much weight or sleeping in a “funny” position, or maybe they have developed arthritis in their neck. Those are statistically the most likely causes and your doctor may rely on heuristics to identify one of those as the diagnosis. However, heuristics may get in the way of your doctor exploring autoimmune causes of neck pain like rheumatoid arthritis or cervical spondylitis or life threatening causes, like heart attack, viral or bacterial meningitis, and cancer to name a few.Rare diseases: Here's another way statistics play a part. A rare disease is one that occurs in fewer than one in two thousand people. That’s 0.05 percent. Diagnostic delay and uncertainty is common for each rare disease because so few people have it. But there are lots of rare diseases, almost 15 thousand. They represent around two-thirds of all diseases. When you add up all the rare disease patients in the United States, they number 30 million. That’s 10 percent of the US population.
I had a friendly math argument with one of my physicians some years back. He initially insisted it was unlikely I had a specific condition because it occurred in less than three percent of the population. “I’ve never seen it in my practice,” he countered. He was looking at the odds of a disease. I replied that given the number of patients he saw annually, that meant that approximately 75 of his patients contracted that disease every year. I suggested that meant he had possibly missed it dozens of times annually. He thought for a moment, then said I made a good point. He tested me and I got properly diagnosed and treated. I triggered his uncertainty by upending his heuristics.Training: Medical schools have not trained doctors to deal with uncertainty, to recognize it, embrace it or communicate it to their patients or colleagues. It’s still a relatively new field in medicine and medical research.
That’s why I want to highlight a short list of remarkable researchers and educators studying diagnostic uncertainty, specifically how medical professionals feel about it, how they’re communicating it, how they should communicate it, and how patients feel about it when a doctor says, “I’m not certain what you have.”
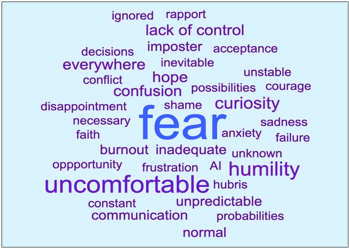
You can follow and check out the work of Maria Dahm, PhD, Traber Giardina PhD, Lekshmi Santhosh, M.D., M.A.Ed., Dimitrios Papanagnou, MD, EdD, MPH, Allyson Bontempo, PhD, and Alexa Miller, whose work in teaching doctors how to communicate uncertainty has resulted in a series of stories featured by a favorite medical podcast The Nocturnists. The Nocturnists shared this word cloud recently. They surveyed 137 clinicians/patients about "Uncertainty and Medicine" and these are the words that came up most.
Fear. Uncomfortable. Humility.
Conclusion
Diagnostic uncertainty happens, it’s a reality, and it can be a powerful tool when doctors and patients are open to its existence. If we can embrace uncertainty and work together as the partners we are meant to be, we can more confidently identify the right diagnosis and the best treatment plan.
It’s important for us as patients to realize that the person in the white coat who seems to have all the power over our medical future is also a human with emotions, stress, fears and hopes, deserving of our courtesy, just as we expect them to treat us with respect.
I’m not suggesting we permit them to dismiss our concerns or symptoms or treat us with arrogance or disdain. Assuming we are conscious and not on a psych hold, we are in control of choosing to engage or not, to walk away or fire them and get a second opinion if our doctors don’t treat us as humans. And if we’re not, our family and friends can advocate for us. Despite the existence of diagnostic uncertainty and error, most doctors are highly educated professionals who have dedicated their whole adult lives to saving ours, and their diagnoses are usually accurate. It’s difficult to recall that when you are one of the patients living in diagnostic limbo or experiencing misdiagnosis. My family has been there, multiple times. Try to remember, they’re not trying to hurt us when they’re failing to help.
My mantra? Embrace uncertainty to reach diagnostic excellence.
© Helene M. Epstein 2024
Great article! Yes, patients need to ask questions but many times they are overwhelmed. However, sometimes when they do ask questions, the medical provider will be rude, dismissive, or act offended. Many people are afraid of making their medical provider mad. In addition, far too often, patients aren't given all the information they need to make true informed decisions thus consent. It is in the best interest of the medical system for patients to simply and blindly follow "doctor's orders". So many doctors and even hospitals invest much time and money into certain training and equipment and they want to make back their investment rather than giving information about other possible forms of treatment. This holds true on diagnosing patients as they have put much time and money into certain diagnostic equipment and need to recoup the associated costs. Patient education is so vitally important and thank you, Helene, for what you do.
I love this writer! This is a remarkably important topic, and one that will affect all of us at one point or another. Far too many people either feel intimidated or overwhelmed by the medical establishment and don't do enough to question, explore options, and demand answers- especially when the answer might be uncertainty.